Enough with the political games. It's time for the minister to listen to the patients instead of the ideologically driven bullies in the NHS.
Ever since Hillary Cass' final report, the only actions that have followed from the government , the various medical organisations involved and the NHS have been designed to create more barriers.
Since it’s publication, the review has been widely criticised and for good reason. Except, if you’re living in the UK you would never know that, on the contrary, you’d probably believe that it was of an exceptionally high standard, so high, that you would want to implement its recommendations without hesitation.
I guess there is one thing that the CASS review has achieved, and that is that it has managed to align all the bigots around the same war cry. It has given air and standing to organisations such as the Society for Evidence-Based Gender Medicine (SEGM), the Clinical Advisory Network for Sex and Gender (CAN-SG) and, the latest addition in fringe organisations European Society for Child and Adolescent Psychiatry (ESCAP). All of them keenly supported by Secretary of State for Health and Social Care, Wes Streeting. It should also not be forgotten that the Labour MP considered a meeting with 5 NHS nurses who’ve decided to take the NHS to court over a trans inclusive changing-room policy. That those 5 ladies are being represented by Christian Legal Centre, the legal arm of Christian Concern. They are an Evangelical Christian Reactionary group with a long and well-documented history of opposing LGBTQ+ equality, abortion rights, gay/lesbian marriage, Islamic Religion and Women’s rights to self-determination.
While Wes was being all smiles, I sat in front of my screen, reading and analysing the inner workings of the Sub-Committee of the Specialist Ad-hoc Research and Ethics Committee. That committee is responsible for keeping scientific studies under review, provide researchers with feedback and recommendations in line with the Research & Ethics Policy. And yes, I have a few things to say about that sub-committee. I’ll get to that further in the article.
First I want to have a word about the medical organisations here in the UK. Since this is the one country where none of the criticism about Cass is ever mentioned. Despite the fact that traditional media and the journalists who work for them flat-out refuse to even mention it, it is now starting to look like there might be some improvement. During the last few months, little by little some news has made it past the borders and, more importantly, Freedom of Information requests have (after a lot of tweaking by many people) led to some more information becoming available. One of the items that I came across were the meeting minutes of the Sub-Committee of the Specialist Ad-hoc Research Ethics Committee (REC). This body is a part of the NHS Health Research Authority. And that committee is especially relevant because they are the same people who have recently provided their judgement on the structure of the new gender dysphoria clinics.
The meeting minutes that I refer to in this article, are all related to the scientific research that the team were performing. Which could very well become the starting point for another article. But let’s not jump the gun yet. First: Introductions!
Composition of the panel looks a bit like a cheap painting but in the end it didn’t matter. I include it mostly so you, the reader, are aware of the expertise in passing judgement. The three sets of meeting minutes, provide with valid insight into the general decision making process of the panel. Additionally, it also helps to evaluate the adequacy of the assessment of evidence which is presented to the panel and conversely shows whether or not there is sufficient push-back to ensure that evidence gets evaluated from different perspectives and that multi-cultural aspects work out authentically. And to ensure how much and which considerations are taken into account to arrive at well-balanced decisions, based on a thorough and complete analysis of relevant sources.
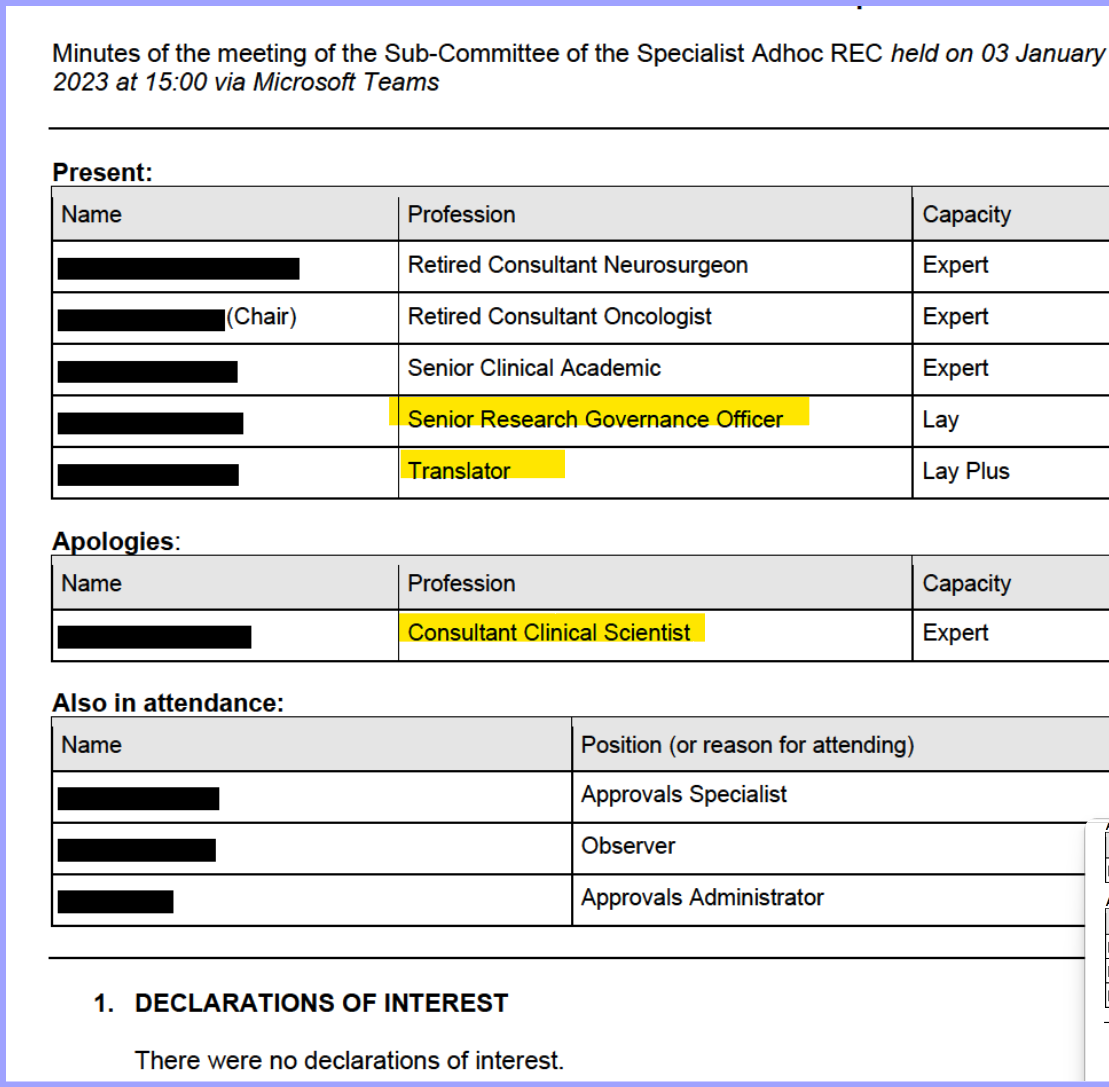
The highlighted roles, refer to Dr Rittakerttu Kaltiala (for the Senior Research Governance Office role) and her translator. The Consultant Clinical Specialist is Dr Hilary Cass.
Before I highlight the concerns I see from this study, let’s first define a few terms. The definitions below are all taken form the Encyclopedia Britannica::
Confirmation bias, people’s tendency to process information by looking for, or interpreting, information that is consistent with their existing beliefs. This biased approach to decision making is largely unintentional, and it results in a person ignoring information that is inconsistent with their beliefs. These beliefs can include a person’s expectations in a given situation and their predictions about a particular outcome. People are especially likely to process information to support their own beliefs when an issue is highly important or self-relevant.
Cognitive bias, systematic errors in the way individuals reason about the world due to subjective perception of reality. Cognitive biases are predictable patterns of error in how the human brain functions and therefore are widespread. Because cognitive biases affect how people understand and even perceive reality, they are difficult for individuals to avoid and in fact can lead to individuals to subjectively different interpretations of objective facts. It is therefore vital for scientists, researchers, and decision makers who rely on rationality and factually to interrogate cognitive bias when making decisions or interpretations of fact. Cognitive A biases are often seen as flaws in the rational choice theory of human behaviour, which asserts that people make rational choices based on their preferences.
A Register of Interests is a record kept, usually by a government body, of financial interests of its members. The register documents interests which may potentially unethically or unlawfully influence members' official duties.
A conflict of interest occurs when an entity or individual becomes unreliable because of a clash between personal interests and professional duties or responsibilities. When such a situation arises, the party with the conflict of interest is usually asked to remove themselves or can be legally required to recuse themselves. These principles and definitions are important to acknowledge and be aware of so that we may hopefully and peacefully discuss where we’re not all aligned.
It is important to acknowledge that the panel discussions follow a set pattern. Their aim is to get a report on the progress of a research study, identify potential issues and evaluate mitigating actions for earlier identified issues. My focus is mostly on verifying that governance processes are adhered to, that people take actions which have a well-informed base and that positive actions are preferred over political interference.
First observation: Going over the set of three meeting minutes, it is noticeable that whenever the research team is challenged on a position or need to answer a query, the clinicians almost unequivocally accept the first remark being made.
Here is the first concern:
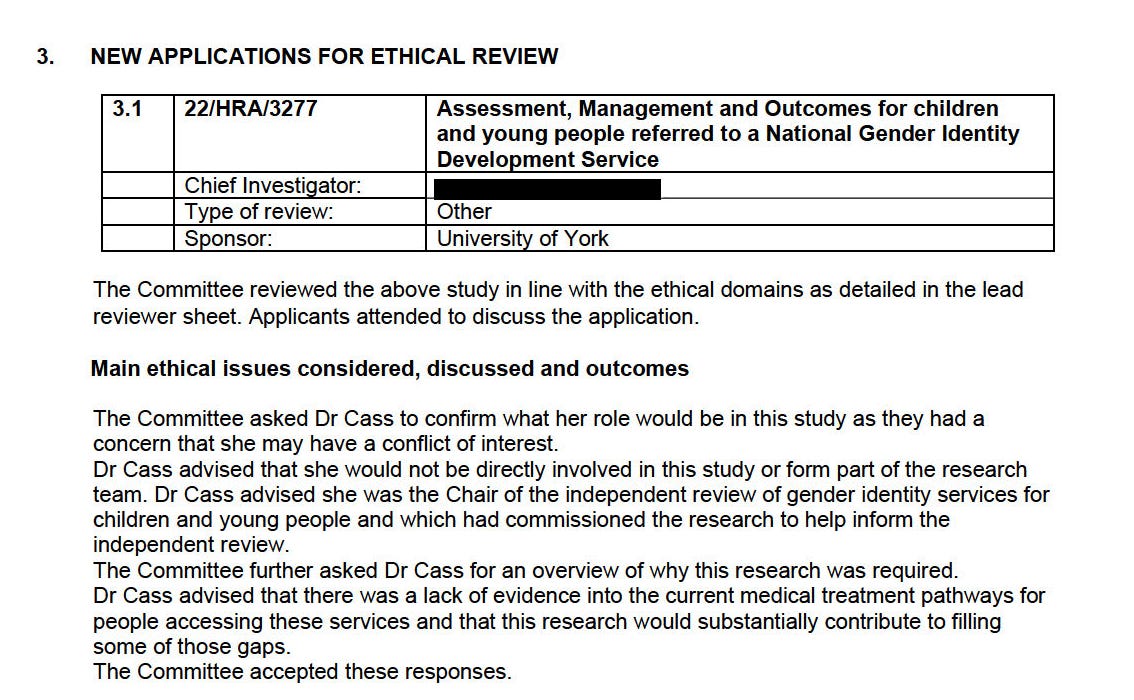
There’s a fair amount to unpack here. Let’s start with the question whether she has a conflict of interest. I’m not at all surprised to read her response. It’s the same approach she takes whenever she’s criticized: Without proper argumentation she simply goes off and says “No”. But what stands out in this case is that she’s already concluded. This conversation took place in August 2022, a little under 2 years before her report is published and yet she has already concluded that there is no evidence and so she will create her own. That attitude comes back in other replies as well. That she made this claim is only part of the problem. That nobody on the review board even thought to challenge her reasoning is inexcusable. The very explanation she uses to deny a conflict of interest, is in fact a conflict of interest because her position isn’t neutral. She’s asking for research to confirm her point of view, ignoring that there could be other reasons: Her last sentence on the evidence informs the panel that the research is only meant to fill in the gaps that she wants.
Then came a real shocker: I did not know this and I honestly don’t think this has ever been mentioned to the general public. Further questions about staff involved in the research bring to light that 2 former staff of the Tavistock and Portman NHS Foundation Trust GIDS are part of the research team. This should NEVER have been allowed. It goes against every ethical standard imaginable. It’s like asking them to grade their own homework.

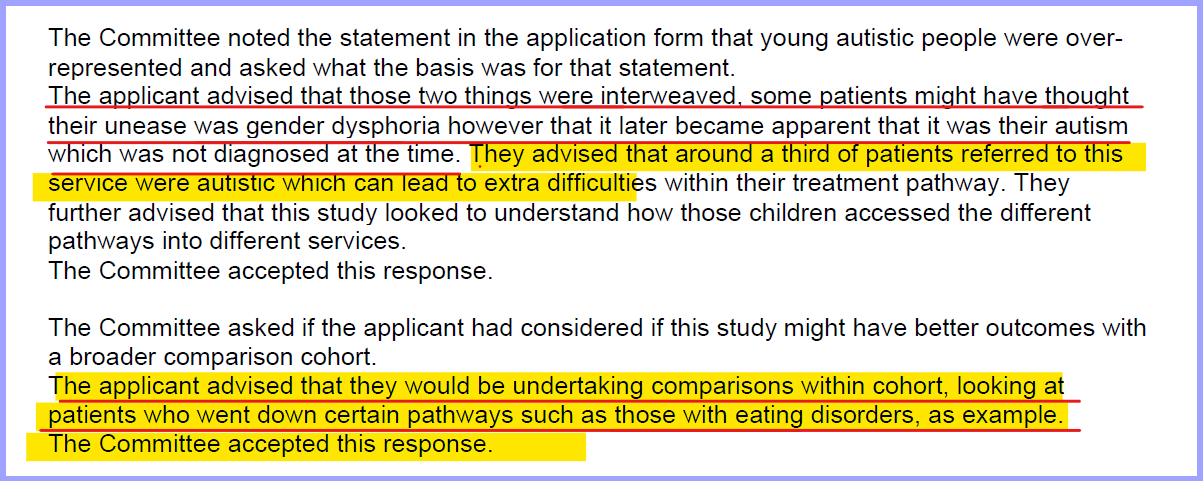
That was swiftly followed with more speculation without evidence, this time referring to an autism spectrum disorder. Which we apparently now can establish without having to test. If I go by the first statement of the applicant, it suggests that they diagnosed the patients in the cohort with autism, based on a single conversation. And then used that argument to claim that one third of all patients were autistic, without providing any basis which would explain causality?
And the real piece de resistance in this section has to be the motivation provided by the applicant when asked to consider expanding their research cohort. How the reply to that question was accepted without any form of challenge, is not something I can approve of. Because not only is the applicant suggesting that gender dysphoria is no different from an eating disorder, we can even follow that treatment plan. Yet another unsubstantiated claim which isn’t at all challenged. In order for such an expansion to be approved, at the very least researchers should establish a correlation between the different datasets. This is clearly not the case. Yet the committee does not even question the reasoning of the applicant over this matter. Seriously, what’s even the point of having that committee if it doesn’t act when needed?